The Problem with the Evidence Pyramid
Originally published: 2025-08-28
A Familiar but Flawed Symbol
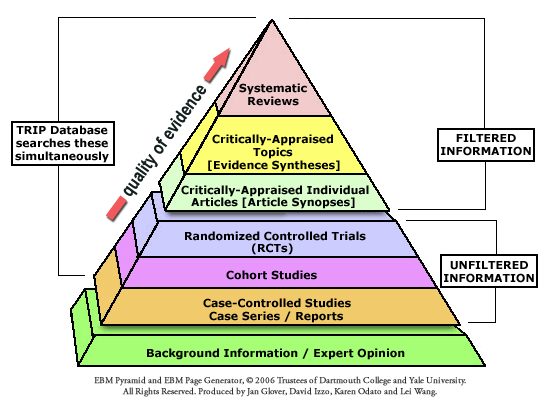
Few images are as instantly recognizable in health care as the “evidence pyramid.” Since the late 1990s, it has been used to show a hierarchy of research designs, from randomized controlled trials at the top down to expert opinion and case reports at the bottom. But as CJ Blunt’s paper The Pyramid Schema shows, the pyramid is more aesthetic than scientific. It oversimplifies, misleads, and strips away nuance in evaluating research quality.
“The pyramid looks authoritative, but it tells us nothing that a simple list or table couldn’t—and it often tells us less.”
What the Research Actually Found
Blunt traces the origins of the evidence pyramid to SUNY Downstate Medical Center in 1997. From there, it spread widely in the early 2000s until it became the visual shorthand for Evidence-Based Medicine (EBM).
But there’s a catch: the pyramid doesn’t improve our understanding of research. Instead, it discourages critical distinctions about study design, quality, and context. Worse, it falsely suggests a rigid, one-size-fits-all ranking of evidence, ignoring the reality that even lower-ranked forms of evidence can sometimes provide stronger insights than higher-ranked ones.
How Chiropractic Has Been Targeted
Within the chiropractic profession, certain factions have eagerly embraced the evidence pyramid to enforce their own narrow version of “evidence-based practice.” By using the pyramid as a weapon, they promote a model of care that prioritizes only randomized trials while dismissing or devaluing observational evidence, clinical experience, and case reports.
This tactic has been particularly harmful to chiropractors who focus on the management of vertebral subluxation. Because research in this area often begins with case reports, case series, and observational designs, pyramid loyalists have used the visual hierarchy to claim such evidence is inherently weak or invalid.
“The pyramid hasn’t just simplified evidence, it has been used to marginalize chiropractic approaches that don’t fit the cartel’s agenda.”
Distorting “Evidence-Informed Practice”
Evidence-informed practice was originally meant to integrate the best available research with clinical expertise and patient values. But the pyramid, when misapplied, creates a distorted version of this philosophy. Instead of encouraging diversity in research methods and clinical approaches, it pushes the profession toward a narrow biomedical model that sidelines chiropractic traditions rooted in vertebral subluxation.
This isn’t just an academic squabble. It shapes policy, influences accreditation and licensure, and reinforces power structures within chiropractic. The pyramid has become a tool for restraint of trade, excluding valid forms of knowledge and practice in the name of “science,” while undermining professional diversity and autonomy.
Moving Beyond the Pyramid
If chiropractic, and healthcare more broadly, is to be truly evidence-informed, it must move past the limitations of the evidence pyramid. More flexible models, like the GRADE framework, already recognize that study quality and context matter far more than rigid design hierarchies. Chiropractic must embrace pluralism in evidence appraisal, ensuring that case reports, clinical expertise, and patient outcomes are respected alongside trials and systematic reviews.
“Real evidence-informed practice values multiple ways of knowing—not just the narrow view dictated by the pyramid.”
Final Word
The evidence pyramid may be iconic, but it has done more harm than good. In chiropractic, it has been used to silence and marginalize, especially those focused on vertebral subluxation. The profession must reject simplistic hierarchies that divide us and instead build a richer, more inclusive vision of evidence-informed care.
